Indications
- Upper extremity fractures
- Lacerations or abscesses of upper arm and deltoid
Contraindications
- Infection overlying injection site
- Allergy to local anesthetic
- Severe lung disease: Risk of unilateral pneumothorax
- Phrenic nerve dysfunction: Specifically contralateral phrenic nerve dysfunction, due to the risk of unilateral paralysis
- Vascular injury/injection: There are many large vessels that serve as landmarks so color doppler and negative aspirations are essential
Equipment
- 20-25cc of local anesthetic of choice
- 18-22G needle
- Saline Flush
- Cleansing solution
- Ultrasound with high-frequency linear transducer
- Ultrasound transducer sterile cover
Prepration
Position
Patient is supine or sitting up with the head turned to the contralateral side. The probe is placed in a parasagittal orientation slightly above the midpoint of the clavicle. Identify the first rib, pleura, subclavian artery, and the brachial plexus directly superficial to the subclavian artery. If the plexus is not clear, fan the probe towards midline or rotate slightly.
Ultrasound
Landmarks
- Place the transducer parallel to the clavicle along the superior border.
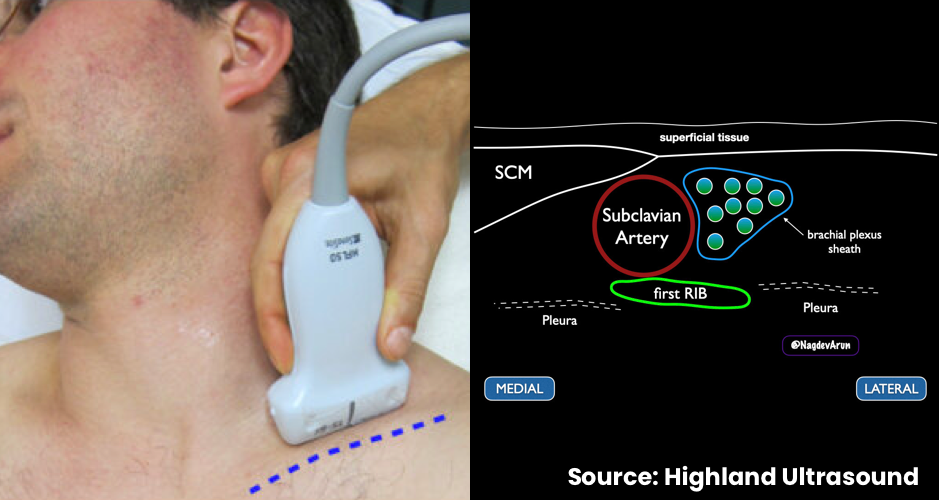
- Locate the subclavian artery (SCA). The brachial plexus will be visible lateral to the SCA.
Technique

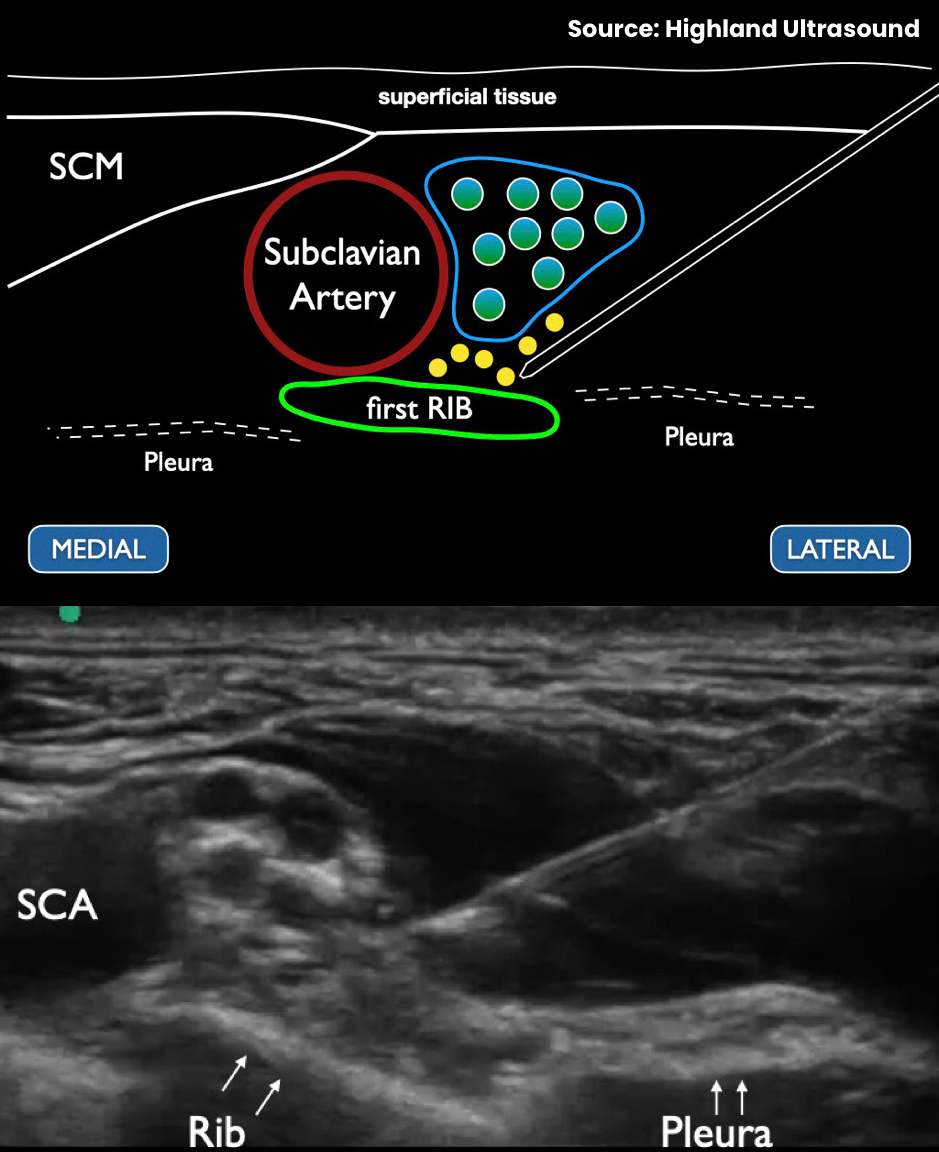
- In-plane needle visualization
- Enter laterally
- A palpable “pop” may be appreciated upon entering the brachial plexus sheath
- Inject 1-2mL of local anesthetic to confirm placement
- Subsequent displacement of the brachial plexus allows further advancement into the sheath by 1-2mm
- Inject remaining local anesthetic
Example