Indications
- Chest wall trauma
- Posterior rib fractures
- Thoracic or abdominal acute herpes zoster or post-herpetic neuralgia
- Vertebral compression fractures
Contraindications
- Infection overlying injection site
- Allergy to local anesthetic
- Requirement for dense anesthesia
Equipment
- 25-30cc of local anesthetic of choice
- 20-22G needle (or spinal needle)
- Cleansing solution
- Ultrasound with high-frequency linear transducer
- Ultrasound transducer sterile cover
Preparation
Position
Expose the posterior thorax by placing the patient prone, in lateral decubitus, or leaning forward in a seated position.
- For the prone position, stand at the head of the bed with the ultrasound machine on either side of the bed
- For the lateral decubitus position (with patient lying on their unaffected side), sit at the side of the bed facing the patient’s back with the ultrasound on the opposite side of the bed
- For the seated position, seat the patient on the edge of the bed leaning forward onto a side table in a position similar to the seated lumbar puncture position. Stand behind the patient with the ultrasound located on the opposite side of the bed anterior to the patient
Ultrasound
Landmarks
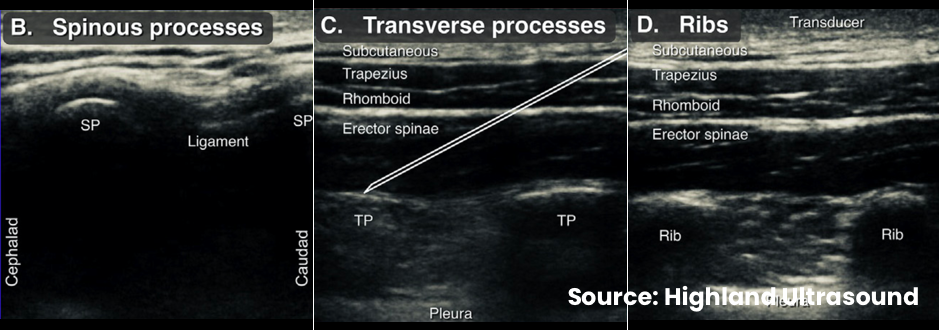
- Begin with the transducer positioned over the midline, oriented vertically – identify the spinous processes
- Translate the transducer laterally to identify the transverse process – the next most superficial bony structure approximately 3cm lateral to the spinous process
- Continue to translate the transducer laterally until the transverse process abruptly disappears and ribs appear, often with more readily-visible pleural line
Technique
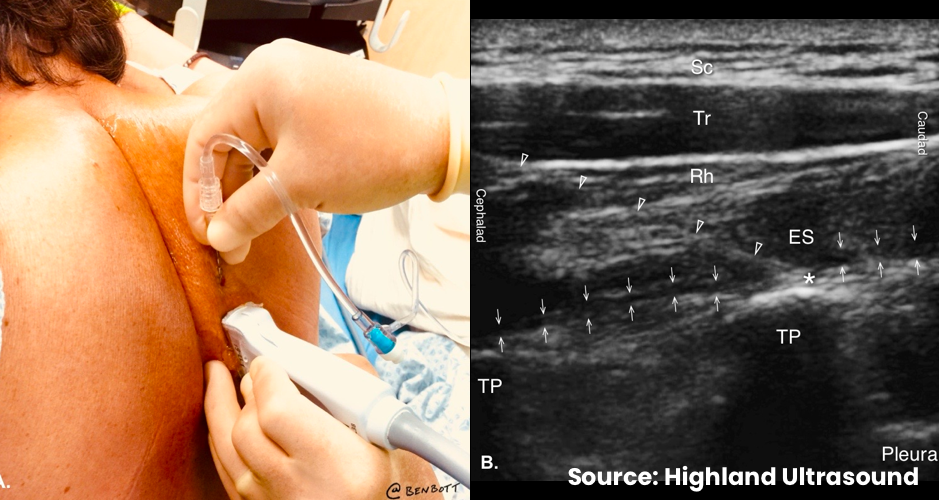
- Identify the targeted transverse process
- Enter in-plane approximately 1-2cm away from the transducer (from either cephalad or caudad)
- Advance the needle at a 30-45° angle towards the posterior surface of the targeted TP
- Feel firm resistance upon contacting the TP
- Aspirate prior to injecting small aliquots of local anesthetic and monitor for separation of the erector spinae muscle from the transverse process, confirming spread within the erector spinae plane
Examples