
Indications
- Upper extremity fractures
- Lacerations or abscesses of upper arm
Contraindications
- Infection overlying injection site
- Allergy to local anesthetic
- Vascular injury/injection: There are many large vessels that serve as landmarks so color doppler and negative aspirations are essential
Equipment
- 15-20cc of local anesthetic of choice
- 22G spinal needle
- Saline Flush
- Cleansing solution
- Ultrasound with high-frequency linear transducer
- Ultrasound transducer sterile cover
Preparation
Position
Position the patient supine with the arm abducted at 90° and externally rotated to expose the axilla.
Ultrasound
Landmarks
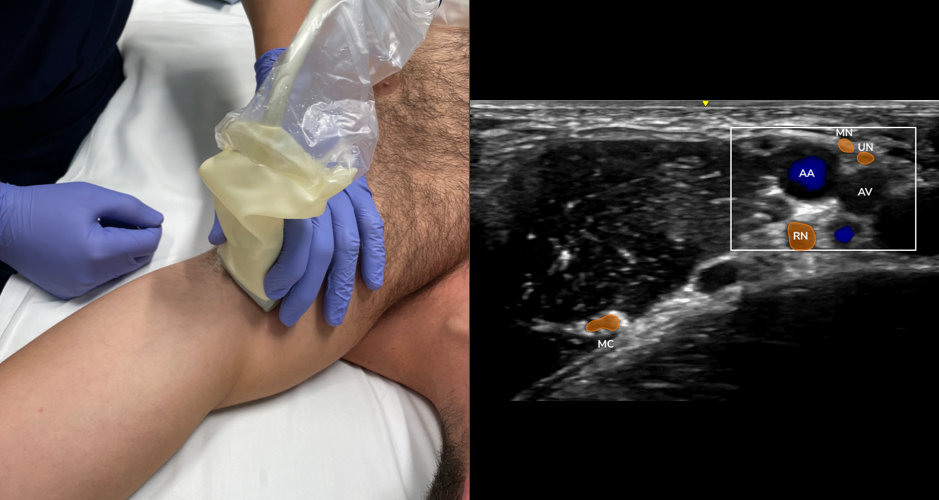
- Position transducer perpendicular to the axis of the humerus and distal to the insertion of the pectoralis major muscle
- Translate the transducer proximally to visualize the axillary artery and surrounding nerves (median, ulnar, radial)
- Important: The axillary region is rich in venous vasculature that is variable in location and easily compressible with light transducer pressure. Thus, the axillary brachial plexus block is susceptible to inadvertent intravascular injection. Care should be taken to apply light probe pressure in order to map vein locations. As always, check for negative aspiration regularly.
- Visualize the musculocutaneous nerve between the coracobrachialis and biceps muscles
Technique
- Plot a trajectory allowing deposition of local anesthetic from a single entry point:
- Deep to axillary artery
- Superficial to the axillary artery
- Between fascial layers of the biceps and coracobrachialis muscles
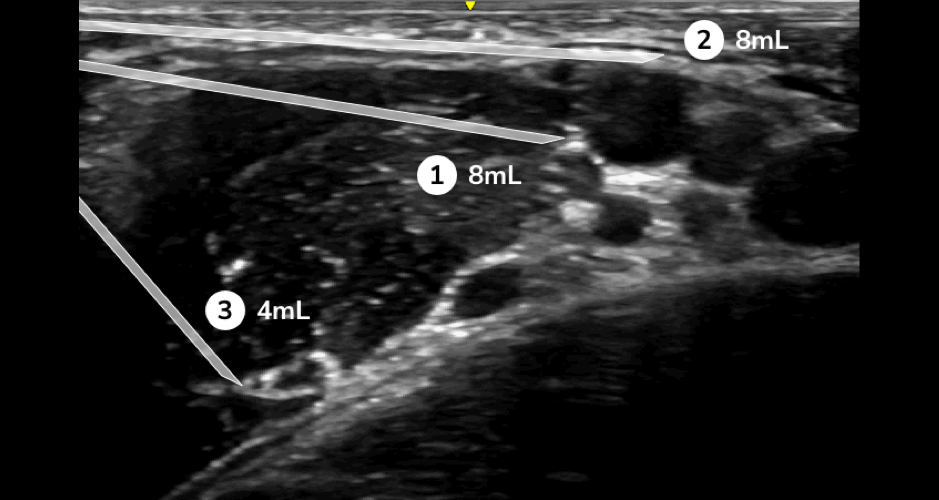
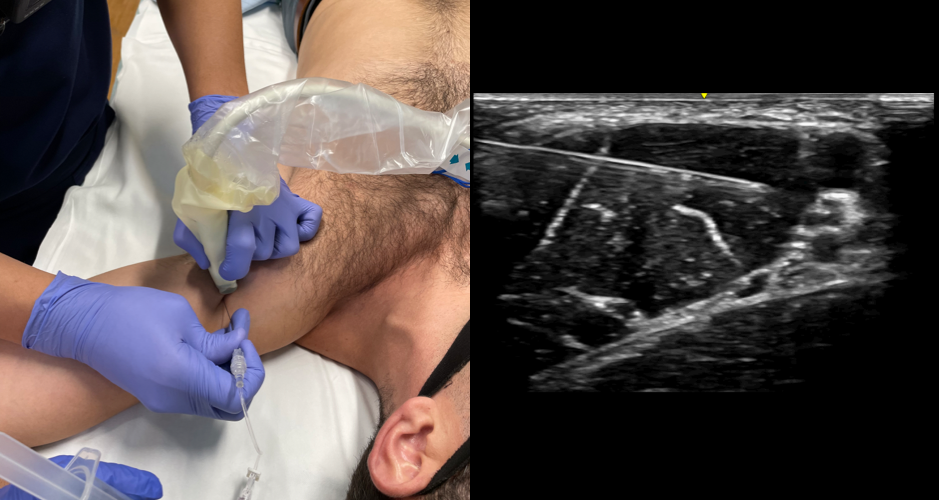
- In-plane needle visualization
- Enter from anterior aspect
- Advance needle deep to axillary artery, deposit 8mL local anesthetic
- Retract, redirect and advance needle superficial to axillary artery, deposit 8mL local anesthetic
- Retract, redirect advanced needle between fascial layer of biceps and corcaobrachialis muscles, deposit 4mL local anesthetic
Examples
Source
- McGovern Medical School Department of Emergency Medicine – Ultrasound Section