Needle Selection
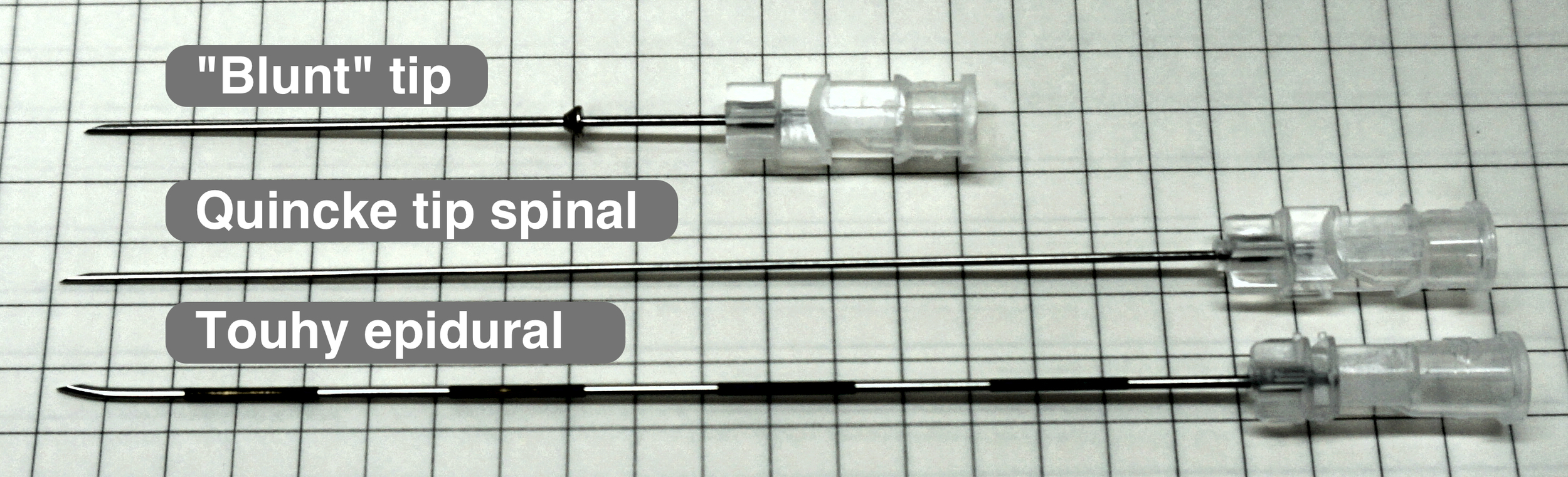
Why blunt?
- Reduced risk of intraneural or worse intrafascicular injection. Likely the primary cause of serious nerve injury from peripheral nerve blocks.
- Reduced risk of intravascular injection and resulting systemic local anesthetic toxicity
- Reduced risk of inadvertent subarachnoid needle placement when performing proximal blocks such as the interscalene brachial plexus block. Total spinal anesthesia and devastating spinal cord syrinx formation has been reported.
- Quincke tip spinal (20-22G) is a back up if a block needle is unavailable
Tips for reducing risk of needle-to-nerve injury
- Only block an awake and calm patient: any paresthesias or pain with needling while using a non-block needle should be be considered high risk events prompting movement away from any nerve, ceasing any injection, and potentially aborting the procedure altogether
- Use in-plane US visualization of the entire needle length
- Avoid high risk blocks (interscalene brachial plexus in particular) unless you have 100% confidence in your needle visualization and anatomy
- Use a stay-away technique maximizing the distance from needle to nerve
- Use hand-on-needle, two-person technique

- Use pressure monitoring
Source
- Highland Ultrasound
Recent Comments